A Summary (for the General Public) and Commentary Regarding the Case Report Published by Dr. Michael Mörz:
Multifocal Necrotizing Encephalitis and Myocarditis
After BNT162b2 mRNA Vaccination against COVID-19
By Rob Rennebohm, MD
November 10, 2022
Take Home Visual images; Take Home Message:
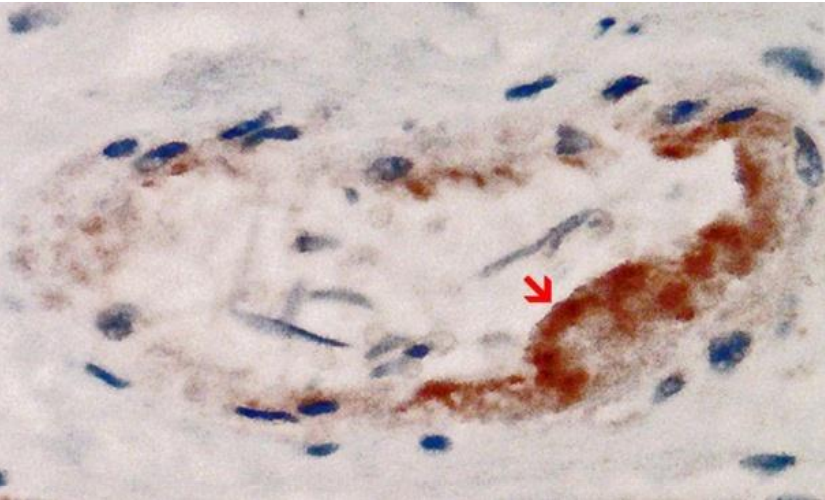
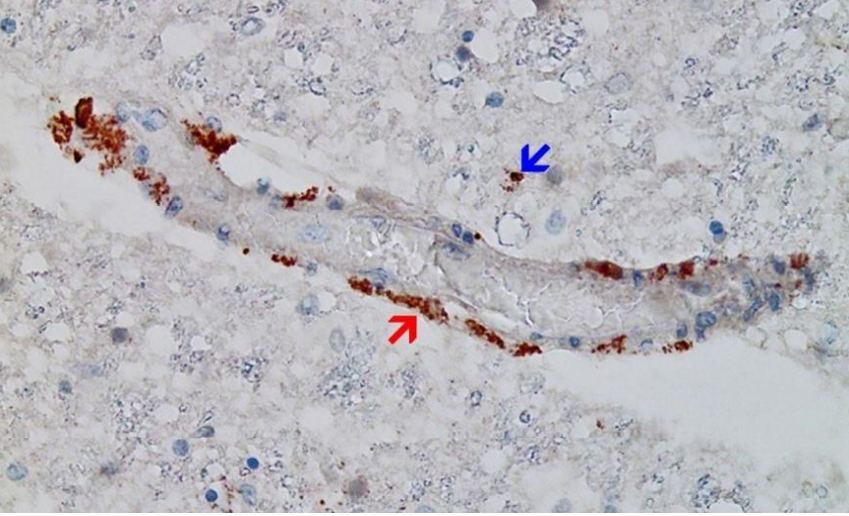
The above image (from the Mörz article: https://www.mdpi.com/2076-393X/10/10/1651) shows a cross section of a capillary in the heart. It demonstrates the presence of an abundant amount of spike protein (the brown material to which the red arrow points) within endothelial cells, which are the cells that line the inner wall of the capillary. There is endothelial cell swelling, and there are a few mononuclear inflammatory cells within the wall of the capillary. The spike protein was demonstrated to be of vaccinal origin, not from SARS-CoV-2 infection.
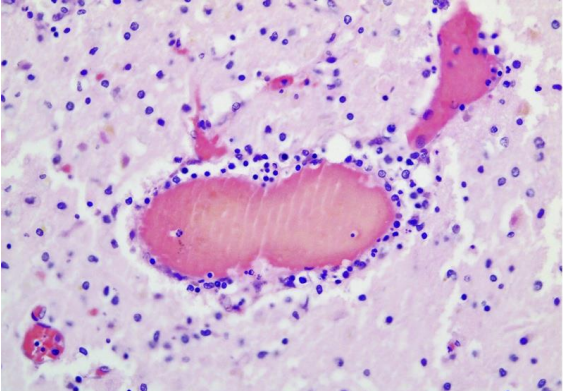
The above image (also from the Mörz article) is a cross section through a capillary in the brain. It shows prominent signs of vasculitis (inflammation of the blood vessel wall). The vessel is filled with hemolyzed blood, which is normal in autopsied cases. The many tiny blue cells that are present in the walls of the vessel (immediately surrounding the hemolyzed blood) include many lymphocytes (inflammatory cells). The presence of numerous lymphocytes in the wall of this vessel means that the vessel wall is inflamed—-i.e., the vessel is experiencing vasculitis.
Take Home Message: As we will discuss in detail below, the above two images (along with the several other images presented in the Mörz article) support the following hypothesis: When the mRNA (that is embedded in the lipid nanoparticle of the Pfizer/BioNTech COVID-19 vaccine) is injected into the arm, the mRNA finds its way (via the blood stream) into distant cells—in this case endothelial cells that line the small blood vessels in the heart and brain. (The vaccine does not simply stay in the arm.) Once in the endothelial cell(s), the mRNA instructs the ribosomes in the cell to manufacture spike protein. The spike protein then migrates to the outer surface of the endothelial cell. The immune system then recognizes the spike protein (or fragments thereof) as foreign and concludes that the endothelial cell has become infected. Accordingly, the immune system sends lymphocytes and other inflammatory cells into the walls of the vessel to attack the presumed infected endothelial cell. The vessel wall becomes inflamed (vasculitis) and, during this process, the endothelial cells become immunologically injured and may swell to varying degrees. Sometimes, abnormal intravascular coagulation (clotting within the vessel) may be triggered. In some instances spike protein may appear within the brain (or heart) tissue, where the spike protein may trigger an inflammatory reaction (encephalitis, myocarditis).
Introduction:
Above is the title page of the article written by Dr. Michael Mörz , a pathologist in Dresden, Germany. Here is the link to the full article: (https://www.mdpi.com/2076-393X/10/10/1651). It is a case report of autopsy findings in a 76-year-old man who had died 3 weeks after receiving his third vaccination against COVID-19. This case report was published by the peer-reviewed journal Vaccines on October 1, 2022 (Vaccines 2022, 10, 1651).
Dr. Mörz’s article provides compelling and sobering evidence of potential serious side effects of the mRNA vaccines. His article may prove to be one of the most pivotal articles to be published in the formal conventional medical literature during the COVID-19 pandemic—because of its potential to change attitudes about the safety of mRNA vaccines against COVID-19.
I will try to summarize the Mörz article and present its pathology images in a way that might be more understandable to non-pathologists and the general public. I will also make further comments about the significance of the Mörz article and what future studies and actions might be helpful to do.
Summary of the Mörz Article:
The Mörz article provides details of an autopsy performed on a 76-year-old man who had died 3 weeks after receiving his third dose of vaccine against COVID-19. He had a past history of Parkinson’s disease. Initially, he had received a single dose of the AstraZeneca vaccine (ChAdOx-1-nCoV-19, a recombinant adenoviral vector vaccine, not a mRNA vaccine), after which he experienced “pronounced cardiovascular side effects.” Subsequently, he received 2 doses of the Pfizer mRNA vaccine (BNT162b2). After the first Pfizer dose, he developed “obvious behavioral and psychological symptoms,” lethargy, and worsening of his overall neurological function. Despite continuation of these symptoms, he was given a second Pfizer dose. Three weeks after his second dose of the Pfizer vaccine, he inexplicably collapsed, was rushed to the hospital, could not be resuscitated, and died. It was thought that he might have aspirated and developed pneumonia (which commonly occurs with severe Parkinsonism). He had never been suspected of having COVID-19, nor had he ever tested positive for COVID-19. Because the cause of death was uncertain, the family requested an autopsy.
After completion of the autopsy, it was concluded that the main cause of death was recurrent aspiration pneumonia. Additional findings, however, included: vasculitis (inflammation of blood vessel walls) within the brain and heart, particularly in small blood vessels (capillaries and arterioles) in his case; necrotizing encephalitis (inflammation of the brain, with associated death of brain cells); and mild myocarditis (inflammation of the heart muscle). These additional findings were thought to be major contributors to his death; they were not thought to be related to his Parkinson’s disease. The final diagnosis was bilateral bronchopneumonia, Parkinson’s disease, vasculitis (in brain and heart), necrotizing encephalitis, and myocarditis.
Among the most remarkable findings were that: the vasculitis, encephalitis, and myocarditis were associated with deposits of spike protein, and the spike protein was vaccinal in origin. As the next several images will show, spike protein was documented to be present within the walls of small blood vessels and also within brain and heart tissue. Inflammatory cells (primarily lymphocytes) were found next to the deposited spike protein. Spike protein could be demonstrated only in the areas with acute inflammatory reactions (brain, heart, and small blood vessels), in particular in endothelial cells, microglia, and astrocytes. The most logical interpretation of these findings is that vaccinal spike protein provoked an inflammatory reaction (by the immune system), resulting in vasculitis, encephalitis, and myocarditis.
It should be added that if vasculitis (inflammation of blood vessel walls) is sufficiently severe, blood flow through the inflamed vessel can be diminished, and this can cause death (necrosis) of the cells that normally receive oxygen and nutrients from blood flowing through those vessels—hence, death of brain cells, for example.
Importantly, Mörz determined that the spike protein came from the vaccine, not from the natural virus. This was concluded because the spike protein was not accompanied by nucleocapsid protein, which is a separate protein located within the SARS-CoV-2 virus. If the spike protein had been of natural viral origin, both the spike protein and nucleocapsid protein should have been present. If the spike protein were of vaccinal origin, spike protein would be present but nucleocapsid would be absent. (The mRNA vaccine instructs the cells to manufacture only spike protein, not nucleocapsid protein.) In this autopsy study, tests for presence of spike protein were positive and tests for presence of nucleocapsid protein were negative.
Glossary:
Before we review the pathology images provided in the Mörz article, let us define key pathological and anatomical terms.
Vascular: This word refers to blood vessels, large and small. The largest blood vessel in the human body is the aorta. In descending order of size, there are large arteries, medium sized arteries, small arteries, arterioles (tiny arteries), and capillaries. In the Mörz article we are primarily talking about arterioles and capillaries.
Vasculitis: When the walls of a blood vessel (large or tiny) are inflamed (meaning that the immune system has sent many inflammatory cells into the vessel walls), the vessel is said to be experiencing “vasculitis.” Many inflammatory cells accumulate on the scene, as if the vessel wall is “infiltrated” or invaded by these cells. Vasculitis can be minimal, mild, moderate, or severe.
Inflammatory cells: Inflammatory cells are key components of the immune system. The immune system sends them to sites of infection, for example, to fight off the infection. Lymphocytes (e.g., T cells and B cells) are key inflammatory cells. Granulocytes, histiocytes, and macrophages are also inflammatory cells.
Glial cells: A type of cell that provides physical and chemical support to neurons (brain cells). Glial cells provide and maintain a healthy, supportive environment for neurons.
Microglia: Microglia is the name given to macrophages that reside in the brain. An important task of microglia is debris clearance. They engulf debris from damaged or dead cells, as well as other debris.
Inflammation: Inflammation is said to be present if an abnormal number of inflammatory cells have accumulated at a site—e.g., within a blood vessel wall (vasculitis), or within brain tissue (encephalitis), or within heart muscle (myocarditis).
Endothelial cells: These are thin elongated cells that line the inner walls of blood vessels. They provide many protective functions and are extremely important.
Endotheliopathy: Disease of (sickness of) endothelial cells.
Encephalitis: Encephalitis means “inflammation of the brain.” It refers to inflammation of brain tissue itself (not inflammation of blood vessels within the brain).
Necrotizing/Necrotic: “Necrotizing” means “capable of causing something to die.” Necrotic cells or necrotic tissue means dead cells or dead tissue.
Necrotizing encephalitis: A severe form of encephalitis—one that is associated with necrosis (death) of brain tissue/cells, including death of neurons (brain cells) and glial cells.
Myocarditis: Inflammation of the heart muscle.
Parenchyma: The functional tissue of an organ, as opposed to the connective and supporting tissue in the organ. In the brain, the parenchyma refers to the “brain tissue,” primarily, the neurons (brain cells) but also glial cells.
Pathogenesis: The sequence of causative processes that lead to disease. The exact mechanisms or chain of events that lead to disease.
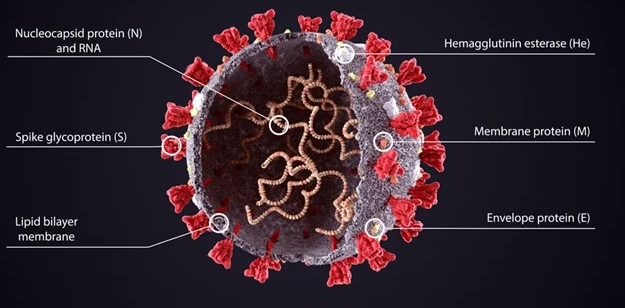
Spike protein: Spike protein is just one of many proteins that are present within or on the surface of the SARS-CoV-2 virus. Spike protein (also called spike glycoprotein) is located on the surface of the virus and enables the virus to enter human cells. The mRNA vaccines instruct cells to make only the spike protein, not any of the other proteins of the SARS-CoV-2. The vaccine provokes the immune system to make antibodies to the spike protein (but not to other proteins of the virus).
Nucleocapsid protein: Nucleocapsid protein is located inside the spherical SARS-CoV-2 virus. It is very different from the spike protein. The mRNA vaccines do not instruct cells to make nucleocapsid protein. Accordingly, the mRNA vaccines do not result in production of antibody to nucleocapsid protein. When a person is infected with the actual virus, both the spike protein and nucleocapsid protein will be present and the person will usually produce antibodies to both proteins. See image below.
Review of Images from the Mörz article:
Instructive images from the Mörz article are shown and discussed below.
I have modified Dr. Mörz’s captions to make them more comprehensible to non-physician readers.
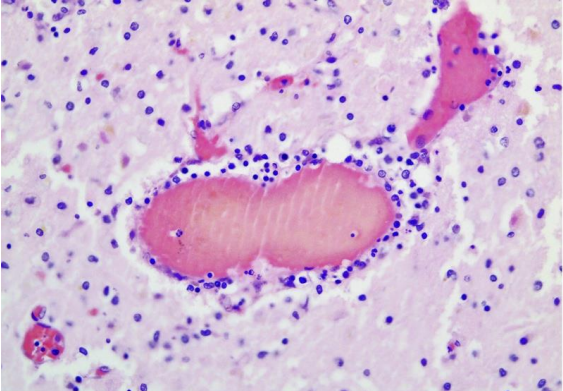
Mörz Figure 4a: Vasculitis (inflammation of the blood vessel wall) in the brain. This is a cross section through a capillary vessel showing prominent signs of vasculitis. The vessel is filled with hemolyzed red blood cells, which is normal in autopsy cases (and, therefore, ignorable). The many tiny blue cells that are present in the walls of the vessel (immediately surrounding the hemolyzed red blood cells) include many lymphocytes (inflammatory cells). So, the walls of this vessel are inflamed, which means the vessel is experiencing vasculitis. The next image provides a closer, more detailed view of the right half of this vessel.
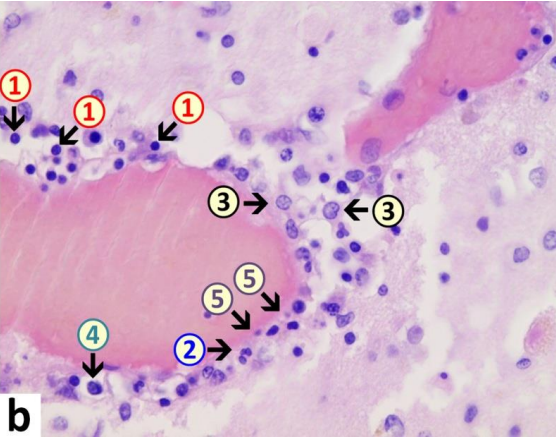
Mörz Figure 4b: Endothelial cells are the cells that line the inner walls of blood vessels. In this image, endothelial cells (5) are swollen and vacuolated and are increased in number with enlargement of nuclei, indicative for activation. Furthermore, within the endothelial layer there is a mixture of different types of inflammatory cells, consisting of lymphocytes (1), granulocytes (2), and histiocytes (4). The adjacent brain tissue also shows signs of inflammation (encephalitis) with presence of lymphocytes as well as activated microglia (3). Lymphocytes are inflammatory cells (such as T lymphocytes). Microglia are macrophages that reside in the brain. A major task of microglia is to engulf and incinerate dead cells. The main finding in this image is inflammation in the vessel wall—i.e. vasculitis.
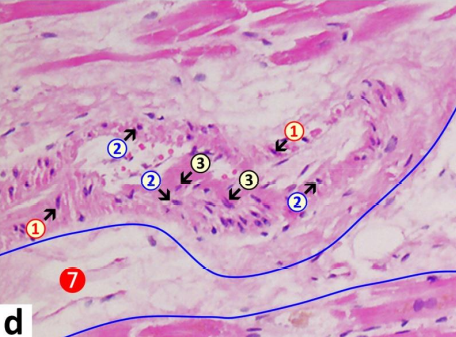
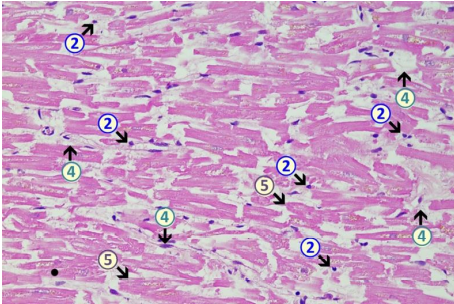
Mörz Figure 5d: This is an arteriole (in the left ventricle of the heart) with signs of inflammation and associated acute degeneration. Lymphocytes (2) have accumulated within the vessel wall; endothelial swelling and vacuolation (3) have occurred; and there is vacuolation of vessel wall myocytes (muscle cells in the wall of the vessel) with signs of karyopyknosis (1). Within the vascular lumen (the open channel of the vessel), note plasma coagulation/fibrin clots adhering to the endothelial surface, indicative of endothelial damage. 1=pyknotic vascular myocytes, 2=lymphocytes, 3= swollen endothelial cells, 4=macrophages, 5=necrotic cardiomyocytes, 6=eosinophilic granulocytes, 7 (blue line)=interstitial edema.
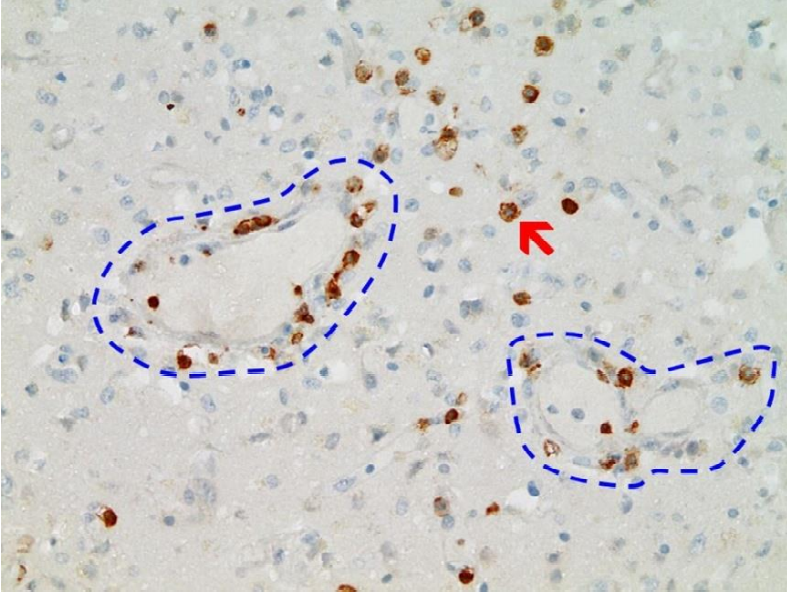
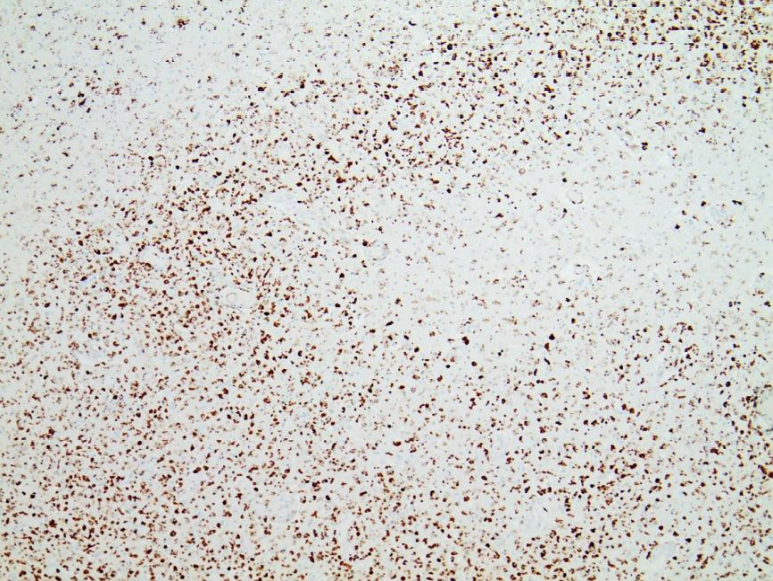
Mörz Figure 8: Frontal brain. Immunohistochemistry for CD3 (expressed by T-Lymphocytes) shows numerous CD3-positive lymphocytes (brown granules, red arrow highlights an example), particularly within the endothelium, but also in the brain tissue, indicative of lymphocytic vasculitis and encephalitis. Blue dotted lines: blood vessels. This image conclusively documents the accumulation of lymphocytes in the vessel wall (vasculitis) and in brain tissue (encephalitis).
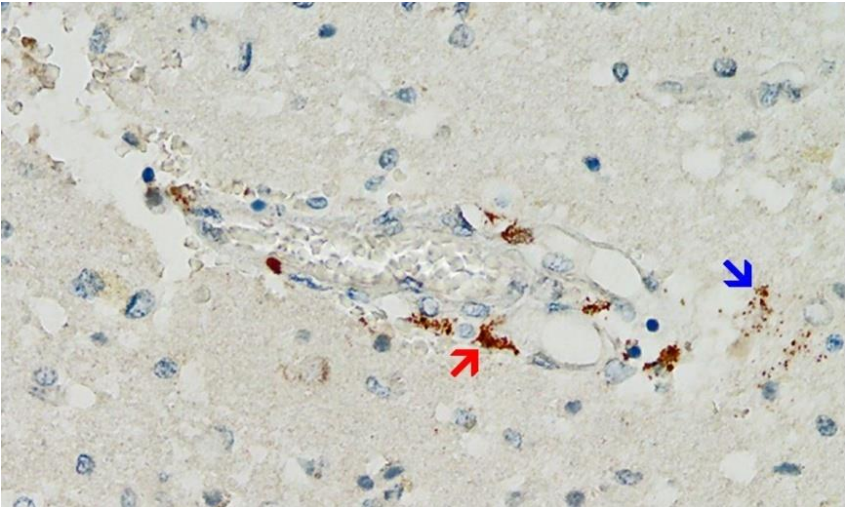
Mörz Figure 9: Frontal brain. Positive reaction for SARS-CoV-2 spike protein. Cross section through a capillary vessel. Immunohistochemical reaction for SARS-CoV-2 spike subunit 1 detectable as brown granules in capillary endothelial cells (red arrow) and individual glial cells (blue arrow). This image conclusively documents presence of spike protein within the vessel wall and in the brain tissue.
Mörz Figure 10: Brain, Nucleus ruber. This image shows the abundant presence of SARS-CoV-2 spike protein in swollen endothelium of a capillary vessel. It also shows acute signs of inflammation with sparse mononuclear inflammatory cell infiltrates in the vessel wall. Immunohistochemical demonstration for SARS-CoV-2 spike protein subunit 1 is visible as brown granules in capillary endothelial cells (red arrow) and individual glial cells (blue arrow). This image conclusively documents presence of spike protein within the vessel wall and in the brain tissue.
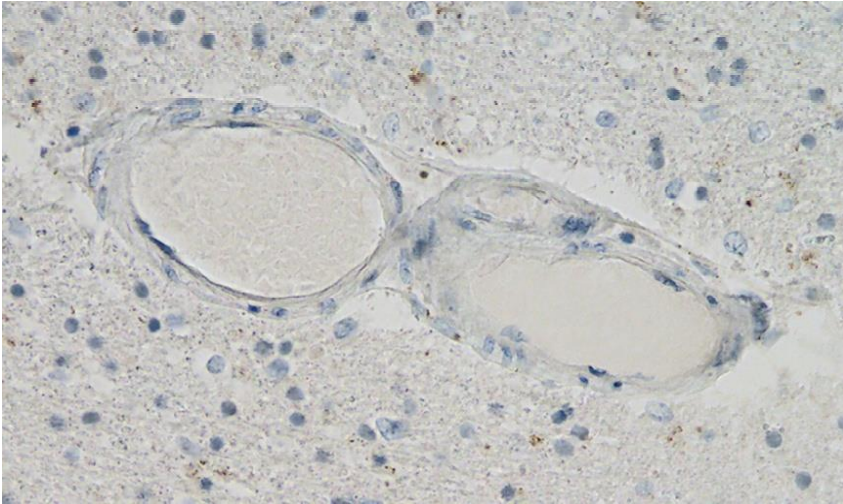
Mörz Figure 11: Frontal brain. Negative immunohistochemical reaction for SARS-CoV-2 nucleocapsid protein. Cross section through a capillary vessel (same vessel as shown in Figure 9, serial sections of 5 to 20 µm). This image documents that nucleocapsid protein was not present, at least in this vessel.
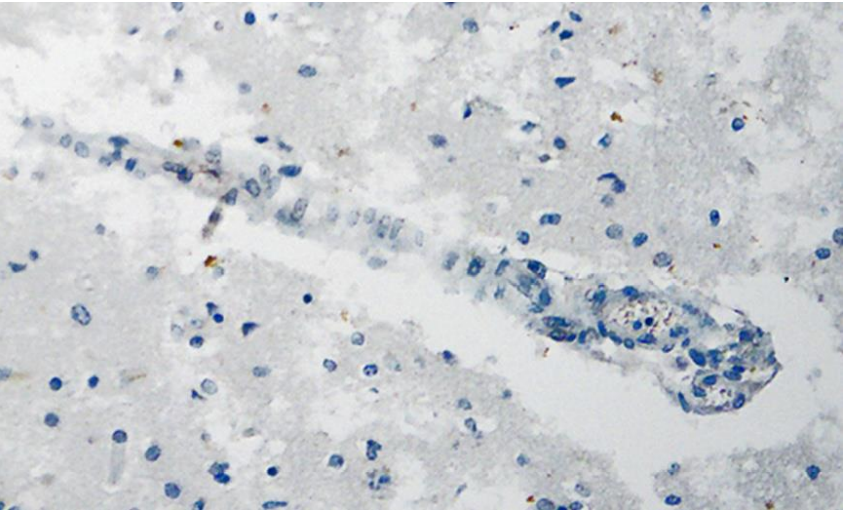
Mörz Figure 12: Brain, Nucleus ruber. Negative immunohistochemical reaction for SARS-CoV-2 nucleocapsid protein. Cross section through a capillary vessel (same vessel as shown in Figure 11, serial sections of 5 to 20 µm). Nucleocapsid protein was not present.
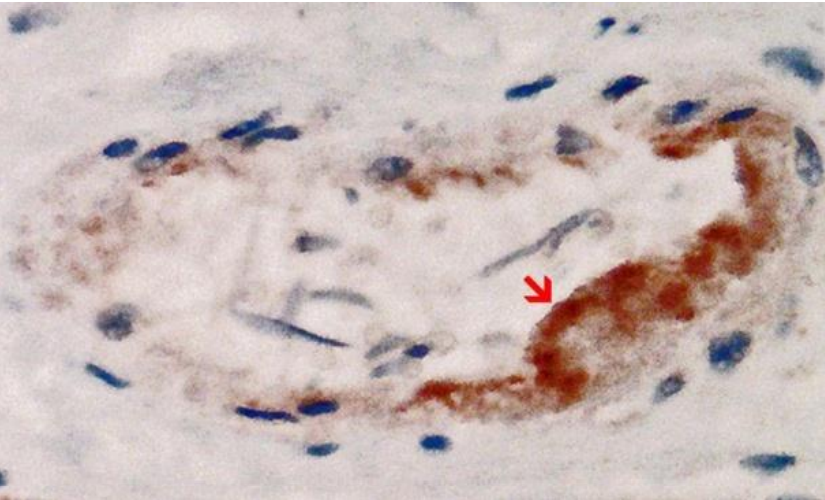
Mörz Figure 13: Heart left ventricle. Positive reaction for SARS-CoV-2 spike protein. Cross section through a capillary vessel (same vessel as shown in Figure 14, serial sections of 5 to 20 µm). Immunohistochemical demonstration of SARS-CoV-2 spike subunit 1 as brown granules. Note the abundant presence of spike protein in capillary endothelial cells (red arrow) associated with prominent endothelial swelling and the presence of a few mononuclear inflammatory cells.
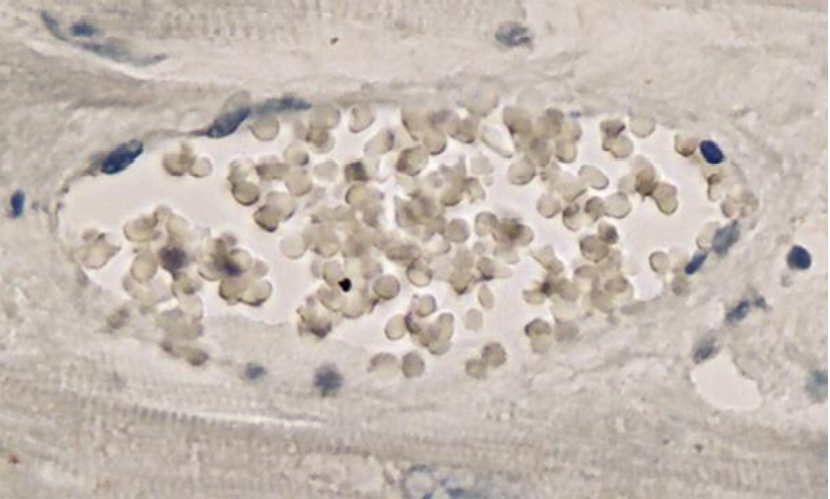
Mörz Figure 14: Heart left ventricle. Negative immunohistochemical reaction for SARS-CoV-2 nucleocapsid protein. Cross section through a capillary vessel (same vessel as shown in Figure 13, serial sections of 5 to 20 µm). Nucleocapsid protein was not present.
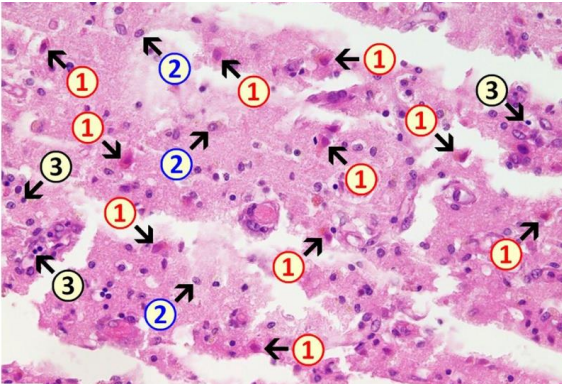
Mörz Figure 2b: Acute brain damage (due to necrotizing encephalitis) is visible with diffuse and zonal neuronal and glial cell death, activation of microglia, and inflammatory infiltration by granulocytes and lymphocytes. 1: neuronal deaths (cells with red cytoplasm); 2: microglial proliferation; 3: lymphocytes.
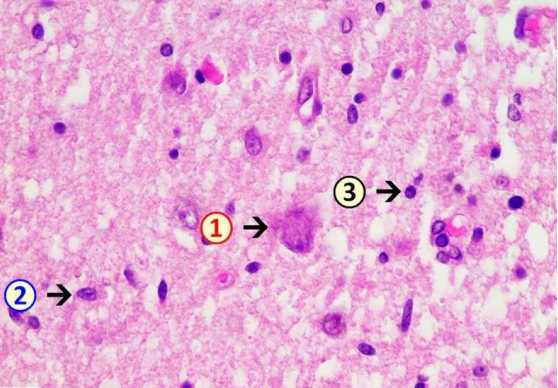
Mörz Figure 3b: Necrotizing encephalitis: Death of neuronal cells is evident and associated with an increased number of glial cells. Note activation of microglia and presence of inflammatory cell infiltrates, predominantly lymphocytic. 1: neuronal death with hypereosinophilia and destruction of cell nucleus with signs of karyolysis (nuclear content being distributed into the cytoplasm); 2: microglia (example); 3: lymphocyte (example).
Mörz Figure 5a: Heart left ventricle. Mild lympho-histiocytic myocarditis. Mild lympho-histiocytic infiltrates (2 + 4). Signs of cardiomyocytic degeneration (5) with cytoplasmic hypereosinophilia and single contraction bands.
Mörz Figure 6: Frontal brain. Diffuse, multifocal necrotizing encephalitis. Immunohistochemistry for CD68 (expressed by monocytic cells). Note map-like tissue destruction with the presence of CD68-positive microglial cells. Furthermore zonal activation of microglia (brown granules). Activation of the microglia means that tissue destruction has taken place in the brain, and macrophages (called microglia in the brain) are clearing/removing the cellular debris. Brown granules: macrophages/microglia.
Additional observations and comments made by Dr. Mörz:
“In some places with inflammatory changes in brain capillaries, there were also signs of apoptotic cell death within the endothelium (Figure 4).
The collective findings were suggestive of multifocal necrotizing encephalitis.
Furthermore, mild acute vascular changes were observed in the capillaries and other small blood vessels of the heart. They consisted of mild lympho-histiocytic infiltrates, prominent endothelial swelling.
Occasionally, adhering plasma coagulates/fibrin clots were present on the endothelial surface, indicative of endothelial damage (Figure 5).
Immunohistochemical staining for the presence of SARS-CoV-2 antigens (spike protein and nucleocapsid) was studied in the brain and heart. In the brain, SARS-CoV-2 spike protein subunit 1 was detected in the endothelia, microglia, and astrocytes in the necrotic areas (Figures 6 and 7). Furthermore, spike protein could be demonstrated in the areas of lymphocytic periarteritis, present in the thoracic and abdominal aorta and iliac branches, as well as a cerebral basal artery (Figure 8). The SARS-CoV-2 subunit 1 was found in macrophages and in the cells of the vessel wall, in particular the endothelium (Figure 9), as well as in the Nucleus ruber (Figure 10). In contrast, the nucleocapsid protein of SARSCoV-2 could not be detected in any of the corresponding tissue sections (Figures 11 and 12). In addition, SARS-CoV-2 spike protein subunit 1 was detected in the cardiac endothelial cells that showed lymphocytic myocarditis (Figure 13). Immunohistochemical staining did not detect the SARS-CoV-2 nucleocapsid protein (Figure 14).
Immunohistochemistry for SARS-CoV-2 antigens (spike protein and nucleocapsid) revealed that the lesions with necrotizing encephalitis as well as the acute inflammatory changes in the small blood vessels (brain and heart) were associated with abundant deposits of the spike protein SARS-CoV-2 subunit 1. Since the nucleocapsid protein of SARS-CoV-2 was consistently absent, it must be assumed that the presence of spike protein in affected tissues was not due to an infection with SARS-CoV-2 but rather to the transfection of the tissues by the gene-based COVID-19-vaccines. Importantly, spike protein could be only demonstrated in the areas with acute inflammatory reactions (brain, heart, and small blood vessels), in particular in endothelial cells, microglia, and astrocytes. This is strongly suggestive that the spike protein may have played at least a contributing role to the development of the lesions and the course of the disease in this patient.
The detailed autopsy study revealed additional pathology, in particular necrotizing encephalitis and myocarditis. While the histopathological signs of myocarditis were comparatively mild, the encephalitis had resulted in significant multifocal necrosis and may well have contributed to the fatal outcome.
In the brain and heart, it appeared that the small blood vessels were especially affected, in particular, the endothelium. In severe SARS-CoV-2 infections, a systemic exposure to the virus and its spike protein elicits a strong immunological reaction in which the endothelial cells play a crucial role, leading to vascular dysfunction, immune-thrombosis, and inflammation.
During an infection with the virus, both proteins should be expressed and detected together. On the other hand, the gene-based COVID-19 vaccines encode only the spike protein and therefore, the presence of spike protein only (but no nucleocapsid protein) in the heart and brain of the current case can be attributed to vaccination rather than to infection. This agrees with the patient’s history, which includes three vaccine injections, the third one just 3 weeks before his death, but no positive laboratory or clinical diagnosis of the infection.
The stated purpose of the gene-based vaccines is to induce an immune response against the spike protein. Such an immune response will, however, not only result in antibody formation against the spike protein but also lead to direct cell- and antibody-mediated cytotoxicity against the cells expressing this foreign antigen. In addition, there are indications that the spike protein on its own can elicit distinct toxicity, in particular, on pericytes and endothelial cells of blood vessels.
Several studies have found the vaccine mRNA and/or the spike protein encoded by it at a considerable distance from the injection site for up to three months after the injection.
Biodistribution studies in rats with the mRNA-COVID-19 vaccine BNT162b2 also showed that the vaccine does not stay at the injection site but is distributed to all tissues and organs, including the brain.
In the case reported here, it may be noted that the spike protein was primarily detected in the vascular endothelium and sparsely in the glial cells but not in the neurons. Nevertheless, neuronal cell death was widespread in the encephalitic foci, which suggests some contribution of immunological bystander activation, i.e., autoimmunity, to the observed cell and tissue damage.
This is the first report to demonstrate the presence of the spike protein within the encephalitic lesions and to attribute it to vaccination rather than infection. These findings corroborate a causative role of the gene-based COVID-19 vaccines, and this diagnostic approach is relevant to potentially vaccine-induced damage to other organs as well.”
Conclusions:
Dr. Mörz has conclusively demonstrated the presence of an abundance of vaccinal spike protein in the endothelial lining of the walls of capillaries and arterioles in the brain and heart. He has also demonstrated significant inflammation within the walls of these same vessels. His interpretations of the findings are appropriate and not overstated. He has appropriately suggested that these two findings are linked—that the inflammation in the vessel walls (vasculitis) was most likely triggered by the presence of vaccinal spike protein in those walls.
Dr. Mörz has also conclusively demonstrated diffuse and multifocal inflammation in the brain tissue (encephalitis) and in heart muscle (myocarditis). The encephalitis was necrotizing—i.e., associated with death (necrosis) of brain cells (neurons). It is difficult to know what was chiefly responsible for the necrosis of the brain cells. The findings do not provide good evidence for a direct immune attack on neurons. It is possible that this necrosis represented collateral damage that occurred while nearby microglia/inflammatory cells dealt with spike protein that had penetrated into the brain tissue. It is also possible that the necrosis was partly due to critically impaired blood flow, due either to partial or complete occlusion of capillaries (due to endothelial cell swelling or accumulation of cellular debris and/or thrombotic material) or to severe injury/obliteration of capillaries—such that brain tissue did not receive sufficient vascular delivery of oxygen and nutrients.
The latter possibility (death of brain cells due to impaired blood flow at the capillary level), may not be detectable without use of electron microscopy (EM). That is, such capillary damage may not be visible upon light microscopic examination and may be detectable only upon examination by EM. In studies of Susac syndrome (SuS), for example, EM has revealed spectacularly abnormal endothelial swelling and damage in brain capillaries (including capillary obliteration) that were not evident on light microscopy.1 (SuS is a rare immune-mediated, ischemia-producing, occlusive microvascular endotheliopathy/basement membranopathy that affects the brain, retina, and inner ear.) Experience with SuS, therefore, raises the possibility that EM studies of possible vaccine-induced brain injury might reveal extensive capillary abnormalities that are not evident on light microscopy. Dr. Mörz’s examinations included light microscopy but not EM.
Taken together, Dr. Mörz findings provide strong support for the following hypothesis: When the mRNA (that is embedded in the lipid nanoparticle of the Pfizer/BioNTech COVID-19 vaccine) is injected into the arm, the mRNA finds its way (via the blood stream) into distant cells—in this case endothelial cells that line the small blood vessels in the heart and brain. (The vaccine does not simply stay in the arm.) Once in an endothelial cell(s), the mRNA instructs the ribosomes in the cell to manufacture spike protein. The spike protein then migrates to the outer surface of the endothelial cell. The immune system then recognizes the spike protein (or fragments thereof) as foreign and concludes that the endothelial cell has become infected. Accordingly, the immune system sends lymphocytes and other inflammatory cells into the walls of the vessel to attack the presumed infected endothelial cells. The vessel wall becomes inflamed (vasculitis) and, during this process, the endothelial cells become immunologically injured and may swell to varying degrees. Sometimes, abnormal intravascular coagulation (clotting within the vessel) may be triggered. In some instances spike protein appears within the brain (or heart) tissue, where the spike protein may trigger an inflammatory reaction (encephalitis, myocarditis) that harms neurons (brain cells) and glial cells.
Vaccinees (and those contemplating vaccination) deserve to know whether the Mörz report of probable vaccine-induced microvascular and parenchymal (tissue) injury in the brain and heart represent extremely rare phenomena or are more common than that. Vaccinees and the public at large deserve to know the prevalence of such phenomena, and they deserve to know the full spectrum of such findings. If such phenomena are more than rare, our hope would be that the abnormalities are usually only minimal, not as dramatic as in the case reported. We would also hope that the abnormalities might be reversible, possibly amenable to treatment—particularly if patients are warned to not receive any further COVID-19 mRNA vaccination.
It would be helpful if autopsies were to be more frequently considered when people have died inexplicably after COVID-19 vaccination and the possibility of vaccine-injury is deemed a plausible contributor to death. For completeness, EM examination would be helpful when such autopsies are performed. (EM has, unfortunately, nearly become a lost art, except with kidney diseases.) Brain biopsy could also be considered in carefully selected patients who are suffering from considerable new, unexplained brain dysfunction that could quite plausibly be due to injury induced by mRNA COVID-19 vaccination.
Our scientific understanding of potential serious complications of the mRNA vaccines—including knowledge of the prevalence, spectrum, pathogenesis, and potential treatment options—will improve if more autopsies (including EM examination when possible) are performed in situations like that of the case reported by Mörz.
Our scientific understanding will also be advanced if the Mörz article is widely distributed and thoroughly discussed among as many physicians and scientists as possible—including those who, heretofore, have promoted mRNA COVID-19 vaccination, as well as those who have challenged the wisdom and safety of the COVID-19 mass vaccination campaign. For example, a simple but helpful next step would be for all academic medical centers, globally, to dedicate a Grand Rounds presentation and discussion (with respectful encouragement of multiple points of view) of the significance of the Mörz article. Such scientific dialogue is an essential fundamental principle of medicine.
It would also be helpful to convene an international panel of representative experts in pathology, neuropathology, neurology, immunology, and vaccinology to carefully, respectfully, objectively, honestly, transparently, and publicly evaluate Dr. Mörz’s findings and the significance of them. If some believe that Dr. Mörz has overstated the findings or has overstated the likelihood of a link between the presence of the vaccinal spike protein and the inflammation in the vessel wall (and in brain and heart tissue), the most helpful and scientifically rigorous way to address such disagreement is to engage in respectful scientific dialogue.
Physicians, nurses, hospitals, medical centers, health departments, the CDC, NIH, FDA, WHO, the pharmaceutical industry, government leaders, and media outlets that have assured the Public that the COVID-19 vaccines are “very safe” (or at least “sufficiently safe under the circumstances”) owe it to the Public to thoroughly, openly, honestly, publicly, and prominently discuss Dr. Mörz’s article and its implications.
To those people who have been encouraged, pressured, even mandated to receive COVID vaccination—physicians and scientists owe a massive top priority collaborative effort to thoroughly study the pathogenesis (the causative chain of events that lead to disease) and potential treatment of vaccine-induced endotheliopathy, vasculitis, encephalitis, and myocarditis—even if these complications prove to be rare. The death of the 76-year-old man reported by Dr. Mörz should not go in vain. We need to determine how to promptly recognize and promptly provide optimal early treatment for vaccinated people who may be developing early evidence of similar complications in their brain, heart, both, and/or elsewhere.
In the meantime we should deeply thank Dr. Mörz for performing and publishing his extensive and careful study of this one patient. The scientific quality of his work is excellent. His careful article represents a major contribution to medicine and Humanity. He is to be commended for the expertise, time, effort, and courage it took to present this compelling and extremely valuable information. He has superbly honored the best traditions of science, medicine, and ethics and has performed a great service to Humanity. We should also commend and thank the journal Vaccines for demonstrating the wisdom and moral courage to publish Dr. Mörz’s article. Like Dr. Mörz, Vaccines has honored the best traditions of science, medicine, and ethics, and has honored Humanity in the process.
Rob Rennebohm, MD
Pediatrician and Pediatric Rheumatologist
Retired (formerly at Cleveland Clinic)
Email: rmrennebohm@gmail.com
Website: www.notesfromthesocialclinic.org
1Dimitri P. Agamanolis, Richard A. Prayson, Negar Asdaghi, Sakir H. Gultekin, Kim Bigley & Robert M. Rennebohm (2019) Brain microvascular pathology in Susac syndrome: an electron microscopic study of five cases, Ultrastructural Pathology, 43:6, 229-236, DOI: 10.1080/01913123.2019.1692117
https://www.tandfonline.com/doi/abs/10.1080/01913123.2019.1692117
0 Comments