APPENDIX OF MEDICAL ILLUSTRATIONS
When a person is exposed to the SARS-CoV-2 virus, the virus typically enters through the person’s nose or throat and threatens to infect the person’s upper respiratory tract (URT). By “threatens to infect” we mean that the virus tries to enter the mucosal cells in the URT. The virus wants to enter those cells because it needs to replicate within our cells in order to survive. Viruses cannot replicate outside of living cells and, therefore, cannot survive outside of cells.
The SC-2 virus is able to enter cells because it has spike protein on its surface that it inserts into the ACE2 receptors on mucosal cells (and, potentially, other cells). When this insertion occurs, the ACE2 “door” of the cell opens and the virus enters the cell. The spike protein is the “key,” and the ACE2 receptor is the “keyhole.” Specifically, and more accurately, it is the Receptor Binding Domain (RBD) at the tip of the spike protein that is inserted into the “keyhole” to unlock the “door.”
Below are many illustrations that will help the reader to better visualize the appearance of the whole virus, the spike protein on the surface of the virus, the RBD at the tip of the spike protein, the ACE-2 receptor on human cells, the NTD (N-terminal domain) of the spike protein (where vaccinal non-neutralizing antibodies attach), and how antibodies bind to the RBD to block its attachment to the ACE-2 receptor.
For a review of how the immune system works, the reader is referred to the second section of the original Open Letter and to the entirety of the Open Letter—Part II.
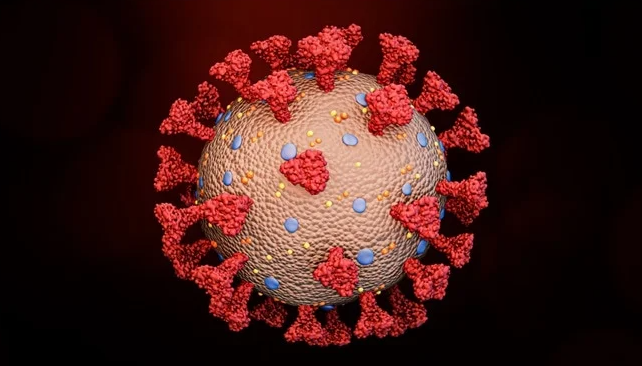
Figure 1: Here is the whole SARS-CoV-2 virus—the entire coronavirus, with many spike proteins (red) projecting from its surface.
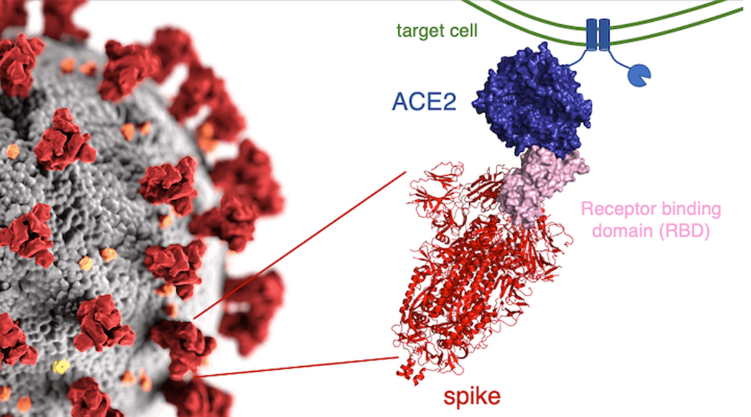
Figure 2: On the left, many spike proteins (red) are sticking out from the surface of the whole virus. To the right of the whole virus is a drawing of what the actual spike protein looks like (in pink and red). At the tip of the spike protein is the Receptor Binding Domain (RBD), in pink. It is the RBD that fits into (or attaches to) the ACE2 receptor. The ACE2 receptor (in blue) is part of the wall of the human cell (the target cell) that the virus seeks to enter. When the RBD (the “key” ) fits into (attaches to) the ACE2 receptor (the “keyhole),” the door into the cell is opened and the virus enters the cell. The two little squiggly parts at the bottom of the spike protein are what anchor the spike protein into the surface of the virus.
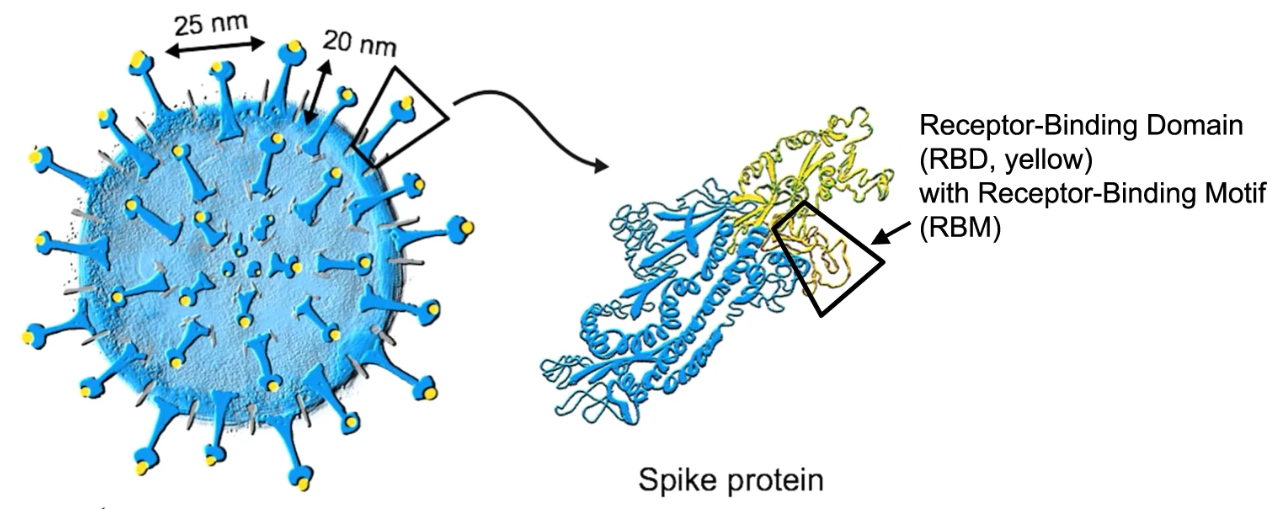
Figure 3: Another view of the whole virus, with its spike proteins. The RBD at the tip of the spike protein is shown in yellow.
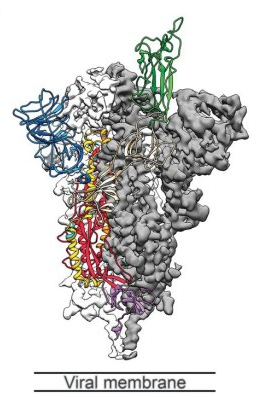
Figure 4: Another drawing of the spike protein. The RBD is shown in green (at the tip of the spike protein). The blue structure in the upper left is the N-terminal Domain (NTD). The gray area represents the lipid membrane of the virus.
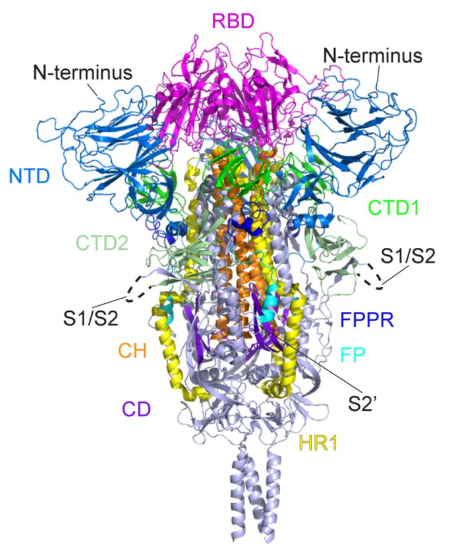
Figure 5: Another drawing of the spike protein. The RBD is at the tip (in magenta). There is an NTD region (in blue) to the left of the RBD and another NTD to the right of the RBD.
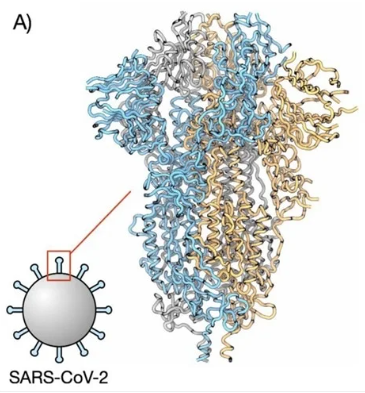
Figure 6: Another drawing of the spike protein.
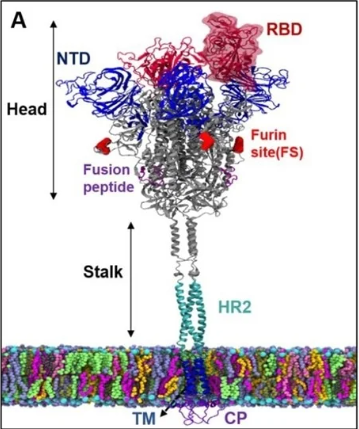
Figure 7: A spike protein anchored within the surface of the virus. The spike protein has a stalk and a head. At the tip of the head is the RBD. An NTD is also shown.
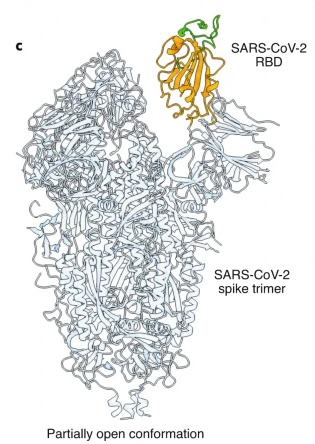
Figure 8: Another drawing of the spike protein. In this drawing the RBD is shown in its “open” position (conformation). When the RBD is in its “open” position, it more easily fits into (attaches to) the ACE2 “keyhole.”

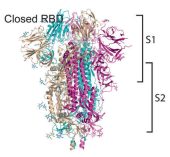
Figure 9: When the RBD is in the “open” position, it is better able to attach to the ACE2 receptor (which is on human cells). When the RBD is in the “closed” position, it is more difficult for it to attach to the ACE2 receptor. Note that the spike protein consists of an S1 region (the upper half) and an S2 region, the lower half. Both the RBD and NTD are in the S1 region.
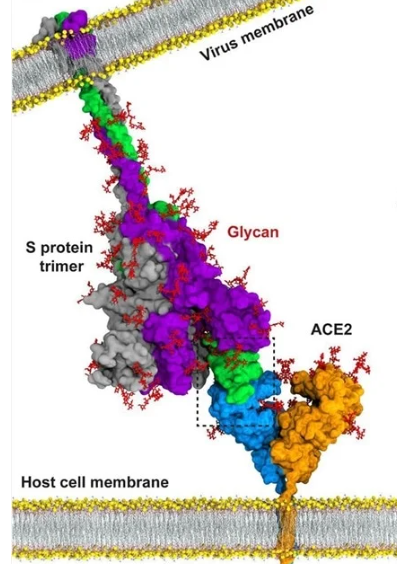
Figure 10: This is a drawing of the spike protein. It is anchored in the outside wall of the virus (the virus membrane). The RBD is shown in green, at the tip of the spike protein. The ACE2 receptor is anchored in the wall (membrane) of the human cell that the virus seeks to enter. The ACE2 receptor is shown with a blue half and a brown half. In this drawing, the RBD is firmly attached to the blue portion of the ACE2 receptor. This attachment will allow the virus to enter the human cell.
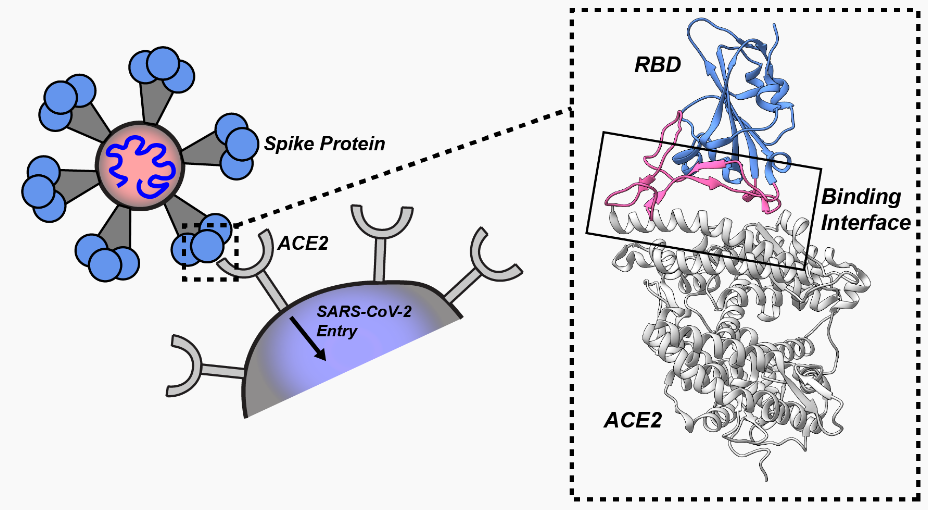
Figure 11: When the RBD (in blue) at the tip of the spike protein fits into (attaches to) the ACE2 receptor (which is on the surface of the human cell that the virus seeks to enter), that attachment results in the virus being able to enter the cell. In the dotted box you can see how the RBD attaches to the ACE2 receptor.
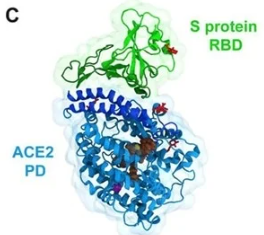
Figure 12: This drawing shows the RBD attached to the ACE2 receptor.
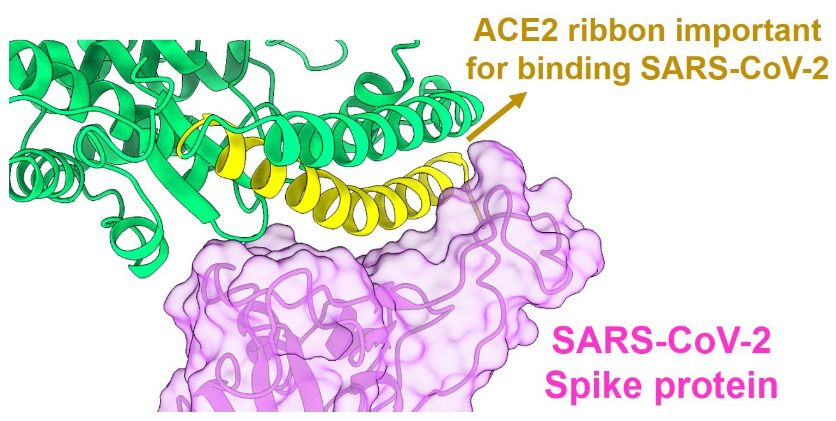
Figure 13: Another drawing of the RBD of the spike protein (in purple) successfully attached to (binding to) the ACE2 receptor (in green).
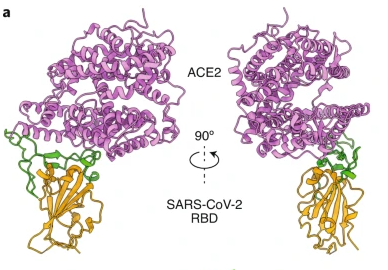
Figure 14: Another view of the RBD (brown and green) bound to the ACE2 receptor (purple).
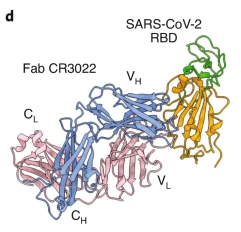
Figure 15: In this drawing a neutralizing antibody (FAB CR3022, blue and pink) has attached to the RBD (brown and green). When an antibody is firmly and tightly attached to the RBD, the RBD will be unable to attach to an ACE2 receptor—i.e., the antibody is neutralizing. The neutralizing antibody blocks the attachment of the RBD to the ACE2 receptor.
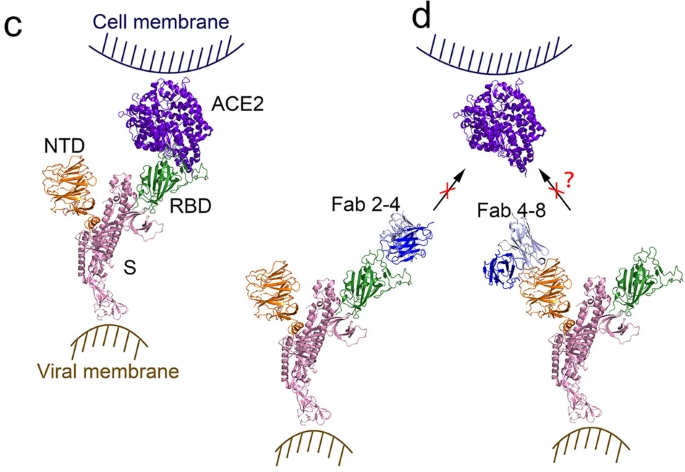
Figure 16: On the left (image C), the RBD at the tip of the spike protein has successfully bound to the ACE2 receptor on the human cell. On the right (image d, note that a neutralizing antibody (Fab 2-4, in blue) has attached to the RBD (in green), and this blocks (prevents) that RBD from attaching to the ACE2 receptor (in purple). Consequently, that virus cannot enter the human cell. On the far right, an antibody (Fab 4-8, in blue) has attached to the NTD (N-terminal domain, in brown) of the spike protein. Early during the pandemic it was suspected that some antibodies to NTD might also somehow block attachment of spike protein to ACE2 receptor—but this was unclear, questionable. Recent studies have demonstrated that, in the absence of effective neutralizing antibodies to the RBD, some antibodies that attach to the NTD can cause conformational changes in the spike protein that result in the RBD moving into an “open” position, and this facilitates RBD attachment to the ACE2 receptor and entry of virus into the human cell. It is now realized that there are antibodies to the NTD that are non-neutralizing antibodies, and that, in the absence of effective neutralizing antibodies, these non-neutralizing antibodies actually facilitate entry of virus into human cells. They do not block entry of virus into cells, they facilitate entry. The COVID vaccines result in production of large quantities of neutralizing antibodies (to the RBD) and non-neutralizing antibodies (to the NTD). When the vaccinal neutralizing antibodies of vaccinated individuals cease to match the mutated RBD of the spike protein of new variants, there is concern that vaccinal non-neutralizing antibodies (to NTD) are able to bind more tightly to the NTD and may facilitate entry of virus into cells. This is why vaccinated individuals may be more easily infected by the Omicron variants that have become resistant to the vaccinal neutralizing antibodies.

Figure 17: This is a drawing of a neutralizing antibody to the RBD of the spike protein. This antibody will block (prevent) attachment of the RBD to the ACE2 receptor.
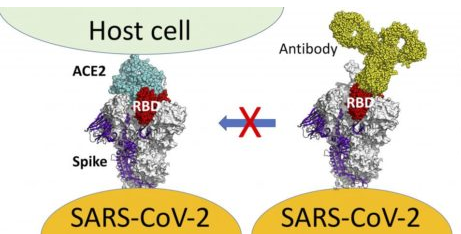
Figure 18: On the left, the RBD at the tip of the spike protein of the virus has successfully and firmly attached to the ACE2 receptor on the human cell. On the right, a neutralizing antibody to the RBD has firmly attached to the RBD. This antibody will prevent the RBD from attaching to the ACE2 receptor.
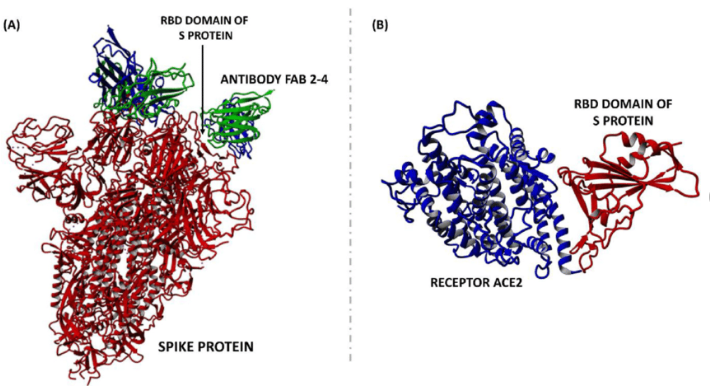
Figure 19: On the left, a neutralizing antibody to RBD (FAB 2-4) has attached to the RBD of the spike protein. This antibody will prevent attachment of the RBD to the ACE2 receptor on human cells. On the right is the usual attachment of RBD to ACE2 that is prevented by neutralizing antibody.

Figure 20: In this drawing, neutralizing antibodies have attached to the RBD of the spike proteins. This blocks attachment of the RBD to ACE2 receptors on human cells. That is how neutralizing antibodies prevent virus from entering human cells.
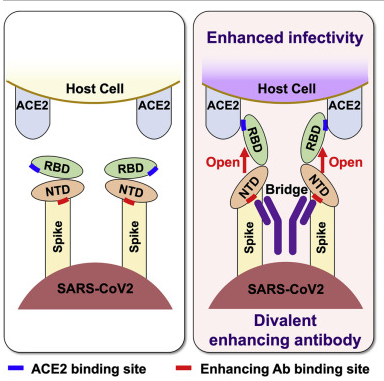
Figure 21: The drawing on the left shows the spike protein (with its RBD and NTD) approaching a human cell. The drawing on the right shows a non-neutralizing antibody (the Y-shaped structure in dark purple) that is attached to the two NTDs. When this non-neutralizing antibody attaches to the NTD, it flips the RBD into the “open” position, which is the ideal position for the RBD to successfully achieve attachment to the ACE2 receptor. In this way, the non-neutralizing antibodies to the NTD actually enhance entry of the virus into the human cell—i.e., increases infectivity.
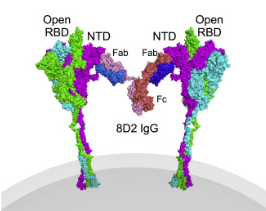
Figure 22: Another drawing of a non-neutralizing antibody (the Y-shaped structure consisting of two Fab fragments and an Fc stalk) that is attached to the NTD of two neighboring spike proteins, resulting in flipping the RBD into the “open” position, thereby enhancing infectivity (viral entry into the human cell).
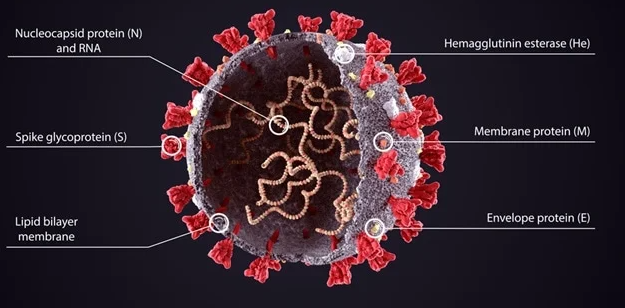
Figure 23: This is the SARS-CoV-2 (SC-2) virus, covered with its spike proteins. Note that there are several other important proteins on and within the virus, besides the spike protein: Nucleocapsid (N) protein, Membrane (M) protein, Envelope (E) protein. The normal, natural immune system wisely produces antibodies not only to the spike protein, but also to many other proteins on/in the virus—including antibodies to nucleocapsid protein. The COVID vaccines train the immune system to produce neutralizing and non-neutralizing antibodies to the spike protein, but not to nucleocapsid protein or other proteins in/on the virus.
Lab testing of people with naturally acquired immunity will reveal antibodies to spike protein and to nucleocapsid protein. Lab testing of people who have been vaccinated and have never had actual natural infection, will reveal anti-spike antibodies but not antibodies to nucleoprotein.
NOTE RE: SOURCES OF MEDICAL ILLUSTRATIONS:
The above Figures 21 and 22 may be found in an article by Liu, et al. at: https://www.sciencedirect.com/science/article/pii/S0092867421006620
All of the other Figures/images (and their sources) may be found by searching for “spike protein N-terminal domain” at:
0 Comments